The assessment by the Joint Committee on Vaccination and Immunisation (JCVI) is that the health benefits from vaccination are marginally greater than the potential known harms. However, the margin of benefit is considered too small to support universal vaccination of healthy 12 to 15 year olds at this time.

Study Reveals Declining COVID-19 Vaccine Efficacy Against Infection
Today’s report tracked the cohort through August 14—incorporating over four more months of data that include a time period in which the Delta variant swept the country—and found that overall, vaccine effectiveness dipped to 66 percent in the weeks when the variant accounted for at least 50 percent of SARS-CoV-2 viruses sequenced. What the study can’t answer is why effectiveness dipped in the weeks dominated by Delta.

[Preprint] Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections
SARS-CoV-2-naïve vaccines had a 13.06-fold (95% CI, 8.08 to 21.11) increased risk for breakthrough infection with the Delta variant compared to those previously infected, when the first event (infection or vaccination) occurred during January and February of 2021.
Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections
Background Reports of waning vaccine-induced immunity against COVID-19 have begun to surface. With that, the comparable long-term protection conferred by previous infection with SARS-CoV-2 remains unclear. Methods We conducted a retrospective observational study comparing three groups: (1)SARS-CoV-…
Ivermectin > Long Known Antiviral Qualities
…cell culture experiments show robust antiviral action towards HIV-1, dengue virus (DENV), Zika virus, West Nile virus, Venezuelan equine encephalitis virus, Chikungunya virus, Pseudorabies virus, adenovirus, and SARS-CoV-2
Ivermectin as a Broad-Spectrum Host-Directed Antiviral: The Real Deal?
The small molecule macrocyclic lactone ivermectin, approved by the US Food and Drug Administration for parasitic infections, has received renewed attention in the last eight years due to its apparent exciting potential as an antiviral. It was identified ...
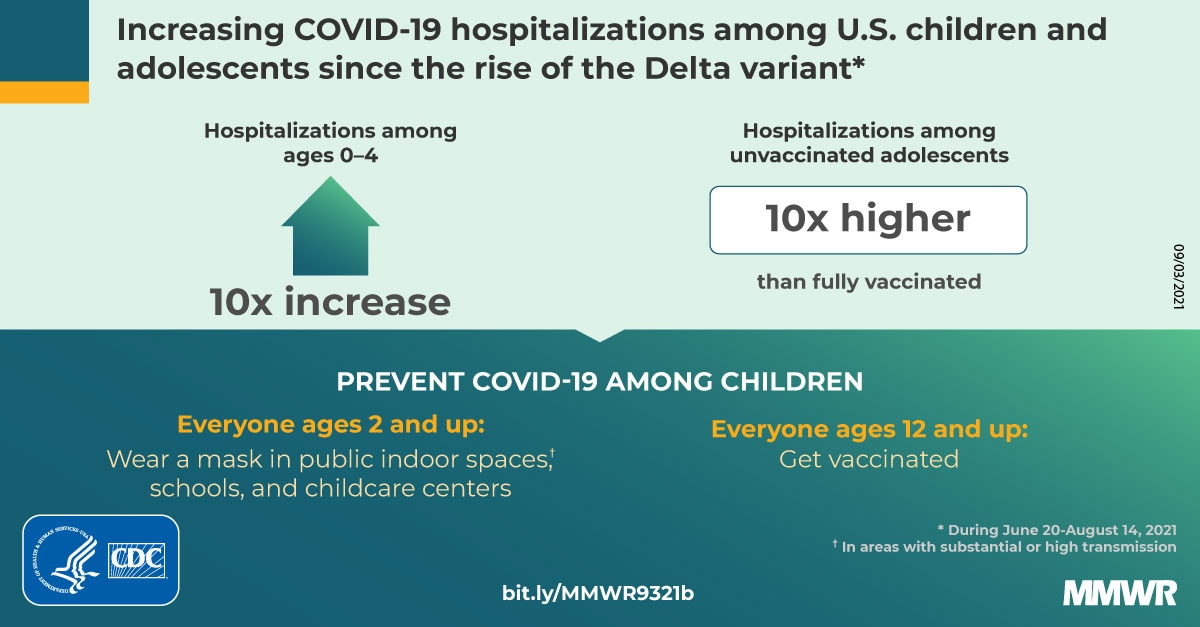
CDC > Hospitalizations Associated with Covid Among Children
COVID-NET conducts population-based surveillance for laboratory-confirmed COVID-19–associated hospitalizations in 99 counties across 14 states. Residents of the surveillance catchment area who received positive molecular or rapid antigen detection test results for SARS-CoV-2 during hospitalization or within 14 days before admission were classified as having COVID-19–associated hospitalizations.
FDA > Emergency Use Authorization
FDA may authorize unapproved medical products or unapproved uses of approved medical products to be used in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions caused by CBRN threat agents when certain criteria are met, including there are no adequate, approved, and available alternatives.

Health Canada > Explanatory note for the Covid-19 Interim Order

Rand Paul clashes with witness

We should be thankful for vaccine passports
We should be thankful for the vaccine passports. The biggest threat to unvaccinated people are VACCINATED people, who are far more likely to be walking around with asymptomatic infections.
Let the self-righteous vaccinated people rule the world for a few months.
We might see them sitting in restaurants or working out at the gym and envy them for now. But soon they will start to realize that they were led astray, and that herd immunity was never even possible with these vaccines.
And we’re certainly not going to envy them when they finally begin to question what an ‘investigatory vaccine’ is, and start to ask themselves why they consented to being injected with one (or three).
And when that happens, we will show them the compassion and understanding that they never showed us.
Do mRNA vaccines stay in the shoulder or travel throughout the bloodstream?
…Compare this to what happens in vaccination. The injection is intramuscular, not into the bloodstream. That’s why a muscle like the deltoid is preferred, because it’s a good target of thicker muscle tissue without any easily hit veins or arteries at the site of injection. The big surface vein in that region is the cephalic vein, and it’s down along where the deltoid and pectoral muscles meet, not high up in the shoulder. In earlier animal model studies of mRNA vaccines, such administration was clearly preferred over a straight i.v. injection; the effects were much stronger. So the muscle cells around the injection are hit by the vaccine (whether mRNA-containing lipid nanoparticles or adenovirus vectors) while a good portion of the remaining dose is in the intercellular fluid and thus drains through the lymphatic system, not the bloodstream. That’s what you want, since the lymph nodes are a major site of immune response. The draining lymph nodes for the deltoid are going to be the deltoid/pectoral ones where those two muscles meet, and the larger axillary lymph nodes down in the armpit on that side.
Now we get to a key difference: when a cell gets the effect of an mRNA nanoparticle or an adenovirus vector, it of course starts to express the Spike protein. But instead of that being assembled into more infectious viral particles, as would happen in a real coronavirus infection, this protein gets moved up to the surface of the cell, where it stays. That’s where it’s presented to the immune system, as an abnormal intruding protein on a cell surface. The Spike protein is not released to wander freely through the bloodstream by itself, because it has a transmembrane anchor region that (as the name implies) leaves it stuck. That’s how it sits in the virus itself, and it does the same in human cells. See the discussion in this paper on the development of the Moderna vaccine, and the same applies to all the mRNA and vector vaccines that produce the Spike. You certainly don’t have the real-infection situation of Spike-covered viruses washing along everywhere through the circulation. The Spike protein produced by vaccination is not released in a way that it gets to encounter the ACE2 proteins on the surface of other human cells at all: it’s sitting on the surface of muscle and lymphatic cells up in your shoulder, not wandering through your lungs causing trouble.
Some of the vaccine dose is going to make it into the bloodstream, of course.
Spike Protein Behavior
I’ve been getting a lot of questions in the last few days about several Spike-protein-related (and vaccine-related) topics, so I thought this would be a good time to go into them. There’s been a recent report about the vascular effects of the Spike protein alone (not coronavirus infection per se), a…